





"We manipulate the finger in extension and simply pop the cord. Now you have a finger that can fully extend, without surgical intervention."—Larry Hurst, MD
In an AAOS press briefing timed to coincide with Auxilium Pharmaceuticals request for expedited approval of the orphan biologic Xiaflex™ (clostridial collagenase for injection), Dr. Hurst explained how the novel treatment works.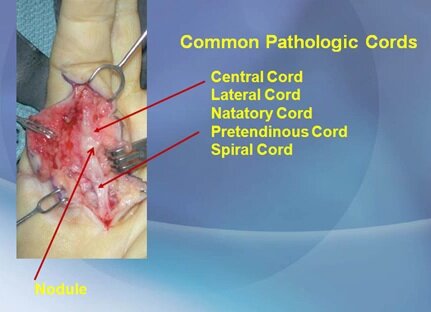
Dupuytren's enzyme treatment offers alternative to surgery
Dupuytren's contracture affects the connective tissue that lies beneath the skin in the palm. Typically, nodules develop in the palm as collagen deposits accumulate, and eventually the deposits form a cord that stretches from the palm of the hand to the base of the finger. The patient's fingers then develop contractures, which progressively impair hand function.
“In Dupuytren's disease the ligaments in the palm become thickened and tumerous. There is a nodular portion with little bumps and a rope-like portion, which is the Dupuytren's cord,” Dr. Hurst said. Although not painful, the disease can be disabling because it can interfere with activities of daily living such as being able to wash your face, put your hand in your pocket, or hold a glass.
Dr. Hurst said that a genetic factor is present in about 40% of cases, with autosomal dominant inheritance with variable penetrance.
"It seems to have gone around the world with the Vikings," Dr. Hurst said. The disease is rare in Africans.
The cord develops from a collagen helix with increased cross-links, increased collagen type III, and other abnormalities, forming an extracellular matrix-cytoskeletal connector.
Traditionally, surgery has been recommended when the contracture is 30 degrees in the MP (metacarpo-phalangeal) joint or 20 degrees in the PIP (proximal interphalangeal) joint. The usual monitoring tool for early-stage Dupuytren's is the table top test. “The patient may present with a little bump on the palm. We tell them to come back when they can no longer put fingers and palm down on flat surface simultaneously,” Dr. Hurst said.
Surgery is usually done under local anesthesia but is not fail-safe. “You cannot get to perfection with surgery. You cannot cure this disease with anything,” Dr. Hurst said.
Consequently, Dr. Hurst and colleagues developed a nonsurgical approach using a tiny injection of clostrial collagenase into the cord to weaken it, followed 24 hours later by manipulation.
"We manipulate the finger in extension and simply pop the cord. Now you have a finger that can fully extend, without surgical intervention," Dr. Hurst said. “Just be very careful not to get collagenase into the tendon.”
The usual collagenase dose is 0.25 cc for MP and 0.20 cc for PIP joints, each cc with 10,000 units of collagenase. Dr. Hurst said that following treatment there is some swelling, but the patient is usually back to fully normal hand function in about one week.
Reference
1. Hurst L. Nonsurgical management of Dupuytren's disease. Press briefing presented at the AAOS 2009 meeting, Las Vegas, February 27, 2009.