





Nonsurgical treatment must not become benign neglect of shoulder separations
Most studies do not show a difference in outcome between surgically and non-surgically treated patients. But non-surgical care may translate into benign neglect, the authors point out. “Perhaps inadequate rehabilitation has been responsible for some of the failures related to nonsurgical treatment,” the study authors write.
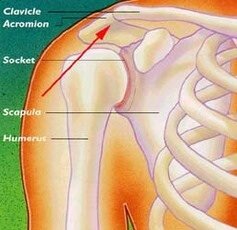 |
| Copyright: American Academy of Orthopaedic Surgeons |
To resolve the disagreement on how best to treat these common injuries, a “well-designed and controlled study comparing people that rehab aggressively versus surgical correction is needed,” Dr. Simovitch told MSKreport.com. “There has not been a prospective, head-to-head comparison of reconstruction versus comprehensive rehabilitation for type III AC injuries and until that exists, there is no compelling evidence one way or the other.”
Type III acromioclavicular joint injuries: Translating research into practice
Certain factors such as symptomology and demand may tip the scale in favor of surgical reconstruction for these relatively common AC joint injuries, Dr. Simovitch said.
For example, overhead athletes and heavy laborers may benefit from surgery for type III shoulder injuries. Moreover, “the younger, more recreationally athletic patient falls into this category as well because they place heavy demand on their shoulders,” he said.
Orthopaedic surgeons who see these injuries should determine what demands are placed on a given patient’s shoulder and to what extent they use their shoulder. “If they are mostly sedentary from a job standpoint, it is a no-brainer to rehab them,” he said. “If a patient has symptoms of pain or mechanical symptoms, lean toward reconstruction, but if they are not symptomatic, try to rehabilitate them.”
Surgeries today are better and safer, he added. Screw fixation of the coracoid process to the clavicle, coracoacromial ligament transfer, and coracoclavicular ligament reconstruction are currently favored for stabilization in cases of acute and late symptomatic instability.
“Biomechanical studies have demonstrated that anatomic acromioclavicular joint reconstruction is the most effective treatment for persistent instability,” the researchers conclude.
References
1. Simovitch R, Sanders B, Ozbaydar M. et al. Acromioclavicular joint injuries: diagnosis and management. J Am Acad Orthrop Surg. 2009;17:207-219.